intoeing
AUTHOR: Marc Mitnick DPM home --> intoeingWHAT IS INTOEING
This problem is not a diagnosis but rather a complaint that usually concerns the parents and results in a visit to the foot specialist. The most important aspect in treating this problem is for the clinician to identify the source of the deformity. A child walking with their feet pointed inward may be caused by a pathological problem within the foot or deviations in normal development in the hip or leg.
does intoeing correct itself?
There is a controversy among medical professionals as to the necessity in treating this deformity. One school of thought is that treatment is not necessary and that the child will eventually outgrow the problem and that any improvement seen in the treatment of the condition is actually the natural resolution of the problem.
Other experts regard pediatric intoeing as an alteration in normal development that can become pathological.
The history of the complaint can be very helpful in pinpointing the source of this inward gait. The age of the child when the condition is first noticed can go a long way in determining the origin of the problem.
AN INWARD FOOT POSITION AT BIRTH is usually the result of a problem directly within the foot.
These include:
- Hallux varus (where the big toe is pointing away from the second toe).
- Club foot
- Metatarsus adductus
- Pes cavus(high arched feet) may all contribute to this problem.
AN INWARD GAIT AT ONE TO TWO YEARS is usually a result of an abnormality in the alignment of the upper or lower leg.
- Tibial torsion- the lower leg is twisted inward forcing the foot to twist inward as well.
- Femoral anteversion- the thigh turns inward and one will notice that not only is the foot twisted inward, but the knee is pointing inward as well.
AN INWARD GAIT BEGINNING AROUND 18 MONTHS may be the result of abnormality in the pelvis or hip region.
One other very important aspect of the child’s history is their neurological status. Factors such as bleeding during early pregnancy, premature labor, difficulty in delivery, and intracranial hemorrhage may all lead to neurological disturbances in the newborn which may manifest itself in one way with intoeing. Neurological disturbances causing this problem will not spontaneously correct itself and more than likely will worsen over time.
If the neurological status is normal then most likely the cause for intoeing is a skeletal abnormality.
It is beyond the scope of this article to discuss treatment for an inward gait as a result of deformity outside the foot.
Most intoeing problems that originate in the foot are congenital meaning they are present at birth. Inspection of the foot alone, at birth, is usually all that is needed to make this diagnosis. As previously noted there are four conditions within the foot that can cause intoeing the most common is metatarsus adductus. The rest of this discussion will deal with this condition.
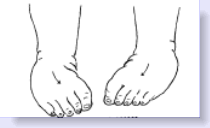
The diagram below (left) demonstrates feet that are directed inward. The problem with this type of deformity is that once the child starts to walk, he or she will have a tendency to trip over their foot (if the condition is severe enough) and the parents will notice that the child is falling more than other children of similar age.
|
|
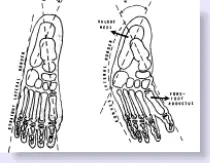
The diagram above (right) shows the skeletal difference between a normal foot on the left and metatarsus adductus on the right.
TREATMENT OF INTOEING
The treatment of choice for metatarsus adductus is serial casting where a cast is applied to the foot and leg in an effort to gently straighten the front of the foot relative to the back of the foot. New casts are applied on a regular basis relative to the amount of improvement noted each time.
The ideal time to institute serial casting is around six months of age, although casting may be beneficial up to two years of age. After age two the success rate drops dramatically. At that point the use of corrective shoes and splints for intoeing may be indicated but their success rate is controversial.
There are no exercises for intoeing, but manual manipulation of the foot may have some benefit.
At one point in time surgical intervention was popular for metatarsus adductus. The main procedure was a soft tissue procedure where ligaments were released in order to allow the forefoot to straighten out. It is not used much today because one of the complications was arthritic changes in the joints where the ligaments were released.
The other surgical option, which is still in use today is abducting metatarsal osteotomies where the metatarsal bones are surgically broken and re-angulated in an effort to straighten out the forefoot. This surgery is reserved for very severe cases of metatarsus adductus.
REFERENCES
Childrens's Hospital of Philadelphia
Massachusetts General Hospital
Want more information? CLICK HERE


Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…