metatarsalgia
AUTHOR: Marc Mitnick DPM home --> metatarsalgiaWHAT IS METATARSALGIA
This is a condition that can best be described as a pain in the ball of the foot, or pain in the metatarsal bones. This condition can have multiple causes. The metatarsal bones are the bones just behind the toes. See the diagram below right.
|

|
As you can see the ends (or heads) of the metatarsal bones bear the body’s weight as the foot moves forward in the gait cycle.
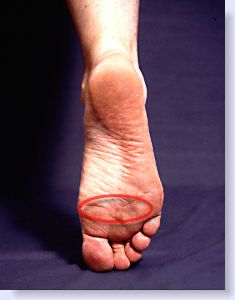
Typically a patient will present to the office complaining of pain in the ball of the foot, (metatarsalgia) many times without any history of trauma. The foot will hurt to walk on sometimes worse barefoot than in shoes. People will come in and complain of symptoms related to a callus (hard skin) that they have on the ball of the foot, asking me to trim it away. Of course, at times calluses can be the source of metatarsalgia, but more often than not the pain is coming from a level deeper than the skin.
conditions that cause metatarsalgia type pain
loss of fat pad- As we age, the one part of the body where we lose fat is the bottom of the foot. Normally the “fat pad” underneath the metatarsal bones cushion the foot. Once this padding is lost a person is then literally walking on the heads of the bones. Doing a lot of walking either barefoot or in shoes with flimsy soles creates a lot of pressure on the metatarsal heads and they begin to hurt thus causing metatarsalgia. A persons foot structure and amount of body weight that they are carrying can also contribute to the problem, as well as occupations that require a lot of standing or walking.
bursitis- Further aggravating metatarsalgia is the fact that in an area of friction or pressure many times the body will attempt to create a cushion to protect the area. This cushion is called a bursal sac. The problem is that as excessive pressure is placed on the bursal sac it too can become inflamed and now is referred to as a bursitis. A patient will typically come into the office complaining of a sharp pain in the foot and will usually be localized to a certain area of the forefoot. In these instances the immediate area may be slightly swollen and slightly red in color.
capsulitis- Other times a patient will present to the office complaining of metatarsalgia type pain that just does not seem to be directly under any metatarsal head. Many times this metatarsalgia pain will be just distal (slightly in front) to the metatarsal heads, almost going into the toe area. In this case we make a diagnosis of capsulitis which is actually a stretching of the ligaments on the bottom of the foot that attach the metatarsal bones into the toes. Specific types of situations which will cause this type of problem include the wearing of high heels which causes excessive stretching of these ligaments, as well as shoes that have very flimsy soles (such as boat shoes) which allow over stretching of the toes as you walk.
Additionally, activities such as climbing ladders where the ball of foot is constantly being jammed into the rungs of the ladder, as well as activities that require a lot of stooping, such as planting flowers, as an example.
neuroma- Along similar lines a patient may present to the office with complaints of a sharp pain which seems to radiate into the toes or back into the foot. There may also be associated complaints of burning and numbness. This can be suggestive of a neuroma or pinched nerve. See the discussion on neuroma.
sesamoiditis- Many times a patient will come into the office complaining of a sharp pain in the ball of the foot that seems to be limited to just behind the big toe joint. The area may also be swollen and feel warm to touch. In this case a diagnosis of sesamoiditis may be made. See the discussion on sesamoiditis.
stress fracture- Lastly, at times a patient may present to the office with pain in the ball of the foot. They may also have a swollen foot and part of the area may be red and very tender to touch. Even though they do not relate to a history of trauma it is very common to sustain a fracture of one of the metatarsal bones. This is more commonly known as a stress fracture and as the name implies, one of the metatarsal bones break as a result of excessive stress being placed on it. I have seen this many times over the years. One would think that it would be limited to older individuals in poor health, but that is not often the case and a stress fracture can and does occur in young healthy individuals as well. See the discussion on foot fractures.
TREATMENT OF METATARSALGIA
Treatment depends on defining the source as discussed above. Generally if the pain is from lack of a fat pad or just too much pressure on the metatarsal heads due factors like obesity or working on concrete floors, adding cushioning and support to the feet through the use of an orthotic should be very effective in reducing pain.
There are even socks made today that have extra cushioning built into them to protect the bottom of the foot and make walking easier.
If a diagnosis of neuroma, bursitis or sesamoiditis is made orthotics may also be very helpful. In many instances a metatarsal pad or metatarsal bar may be added to the orthotic in an effort to take pressure off of the metatarsal heads. Either type of padding may be built into the top of the orthotic and will be placed just behind the metatarsal heads.
In addition, anti-inflammatory medication or cortisone injections may be used as short term therapies. I do not recommend anti-inflammatory medication as a long term solution. Click here for my reasons for not using long term anti-inflammatory medication.
REFERENCES
Want more information? CLICK HERE


Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…