- Home
- tarsal tunnel
tarsal tunnel syndrome
Tarsal tunnel syndrome occurs when the posterior tibial nerve becomes compressed as it passes through a narrow space on the inside of the ankle called the tarsal tunnel. This tunnel is bordered by bone on one side and a thick ligament (the laciniate ligament) on the other, leaving little room for swelling or structural abnormalities.
When the nerve becomes entrapped, swelling and scar tissue reduce its blood supply and impair its ability to glide with ankle motion. This leads to burning, tingling, numbness, or shooting pain on the bottom of the foot. Symptoms may worsen with standing or walking and may vary depending on which branch of the nerve is affected.
Common causes include trauma, excessive pronation that increases tension on the inside of the ankle, tendonitis of structures passing through the tunnel, or space‑occupying masses such as ganglion cysts or lipomas. Diagnosis is based on symptom distribution, tenderness behind the medial malleolus, a positive Tinel’s sign, nerve conduction studies, and imaging when a mass is suspected.
Treatment focuses on reducing pressure on the nerve. Orthotics help when over‑pronation is the underlying cause, while bracing or casting may be used after trauma to limit ankle motion. Anti‑inflammatory medication, corticosteroid injections, and nerve stimulation may provide relief. If conservative care fails, surgical release of the laciniate ligament and removal of any compressive tissue may be necessary to prevent permanent nerve damage.
Reviewed by: Medical Review Board
WHAT IS A TARSAL TUNNEL
Tarsal Tunnel Syndrome is the compression of the main nerve (posterior tibial nerve) that passes under the medial or inside part of the ankle. Peripheral nerves such as the nerves in the feet are richly endowed with their own blood supply and have the ability to stretch or shorten along with the movement of the accompanying joint; in this case the ankle joint.
When the nerve is entrapped in its tunnel the swelling that occurs around the nerve and the ensuing scarring of the nerve inhibit blood flow to the nerve. As the ankle joint continues to move the nerve is further compressed and the ability of the nerve to properly function is diminished.
tarsal tunnel anatomy
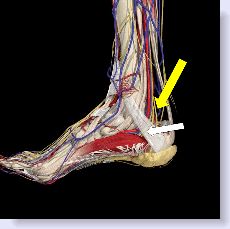
The tarsal tunnel location is on the inside portion of the ankle, just below the medial malleolus, (the bone on the inside of the ankle.)
Below is an anatomical diagram of the band, known as the laciniate ligament represented by the white arrow pressing against the nerve, while the yellow arrow is pointing to the nerve itself.
|
what causes tarsal tunnel
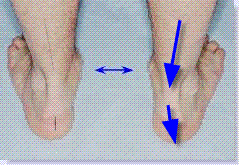
Causes of this syndrome include trauma such as a fall, acute or chronic pronation of the foot that creates excessive pressure on the inside of the ankle. Additionally, a tendonitis of the tendon that passes through the tunnel can create similar symptoms because as the tendon swells it creates excessive pressure within the confined area putting pressure on the nerve. A Below is an example of pronation. See how the arch has collapsed. This creates excessive tension on the inside of the ankle thus causing pressure on the nerve.
Symptoms include burning or numbness usually on the bottom of the foot. It may be worse when standing or walking. There may also be muscle weakness of the muscles that run through the bottom of the foot. The distribution of pain or numbness is dependent on which nerve branch of the posterior tibial nerve is most affected. For that reason all of the foot or only certain parts of the foot may be affected.
Diagnosis is made by the history of the pain or numbness in the area of the distribution of the nerves on the bottom of the foot. Tenderness may be noted over the nerve just behind the ankle joint. Tapping with a finger may send sensations both forward into the foot and backward up the leg; this is known as a positive Tinel's sign. Your foot specialist should be able to determine the distribution of numbness with simple tests. There may also be muscle weakness particularly in the inability to bend your toes in a downward fashion.
Your foot specialist may also order an electromyogram (EMG) which may reveal decreased nerve conduction across the tarsal tunnel. If your doctor feels there may be a soft tissue mass, he may order an MRI.
The Kinoshita test is a pronatory "stress test". Your doctor may attempt to bend your foot upwards and at the same time pronate the foot. The foot is held in that position for ten seconds. At this point, if you have tarsal tunnel syndrome, you will start to feel the symptoms. This test was developed in 2002 and in the initial study after the patients went on to have surgery, the effectiveness of the test was confirmed in 42 out of 43 feet.
Other foot conditions may mimic the symptoms of this condition. These may include radiculopathy (nerve impingement in lower back), diabetic neuropathy, peripheral neuropathy, rheumatoid arthritis, vascular disease, Baxter's nerve (heel neuroma), plantar fasciitis, scar tissue from previous trauma or surgery, ankle edema (swelling) and possibly a growth like a ganglion cyst, or lipoma (fat tumor) in the canal.
An orthotic will prevent the foot from over pronating and thus relieve the pressure on the nerve. Click here for a discussion of tarsal tunnel and orthotics.
If the origin of the problem is traumatic in nature, a tarsal tunnel brace may be indicated as the brace or in many instances, a walking cast, will prevent the ankle from moving at all and will allow the inflammation in the tarsal tunnel to subside.
Adding a heel lift to the walking cast can be helpful as the slight plantarflexion that is created also helps reduce the tension and pressure on the affected nerves.
Along with the above treatments your foot specialist may also prescribe oral anti-inflammatory medicine to help reduce the inflammation.
A tarsal tunnel injection of corticosteroid may also be beneficial.
Transcutaneous nerve stimulation may be helpful as a supplemental treatment as long as the underlying cause of the tarsal tunnel is being addressed.
Other then trying an orthotic that you may purchase, there is very little you can do to remedy your symptoms. Additionally, there are no exercises which will help and actually too much exercise may aggravate your symptoms.
If none of the conservative avenues work then you must consider surgical intervention. Aside from the existing symptoms, if the pressure is not removed from the nerve, the nerve will eventually fail all together making it almost impossible to walk. The surgery itself is a soft tissue procedure whereby the ligament band pressing on the nerve is incised; the posterior tibial nerve is freed from all constricting bands.
This is an out-patient procedure. You will usually require a walking cast. However, prior to consenting to surgery other causes of these symptoms should be ruled out. These include diabetic neuropathy, a pinched nerve in the lower spine, alcoholism, rheumatoid arthritis and heavy metal neuritis just to name a few.
This is a soft tissue procedure that can be performed on an out patient basis. An incision is made just underneath the inside of the ankle bone. The laciniate ligament is a ligament that binds or holds all the vessels and nerves as they pass under the ankle joint. This ligament is incised in an effort to release the pressure that is pressing on the posterior tibial nerve which is causing the tarsal tunnel symptoms.
In addition to releasing the ligament, the area is inspected for the possibility of a growth such as a ganglion cyst which may also be causing pressure on the posterior tibial nerve. Any adhesions (fibrotic tissue attached to the nerve) is also dissected away thus freeing up the nerve.
The skin is closed. The patient may or may not be placed in a walking cast based on the preference of the surgeon.
REFERENCES
The New England Journal of Medicine
The American Journal of Medicine
Q: I am a 70-year-old male with persistent heel pain (14 months) that feels like contact pain. I’ve tried orthotics, steroids, a fracture boot, and PT with no help. One doctor diagnosed Baxter's nerve and recommended surgery; another eliminated it with a lidocaine injection and suggests RSWT. Is surgery with only a 50% success rate the right move? A: When a diagnosis is not definitive, surgical intervention is generally not the first recommendation—especially when the success rate is cited at only 50%. Baxter's nerve entrapment and Tarsal Tunnel Syndrome are two distinct conditions located in different areas of the heel. Recommendation: I suggest a "diagnostic experimentation" phase. By treating one condition conservatively at a time, you can isolate which one responds. If your symptoms subside with one of these targeted conservative treatments, you'll have the confidence of a final diagnosis before ever considering elective surgery. — Marc Mitnick, DPM
Visitor Name: Lynne Hi Lynne, The first thought that comes to mind is to give your situation some more time. Think about it. If you have a nerve entrapment as a result of your feet flattening out and putting pressure on the nerve, just by getting into an orthotic your symptoms should improve, but probably slowly. The tibial nerve is inflamed from the excess pressure, you have now removed the pressure but it takes time for the inflammation to subside. An analogy would be an ankle sprain, you fall and twist your ankle, the ankle hurts and even though you are no longer falling, the ankle still hurts, but, gradually gets better until there is no pain. I would suggest to you that by continual wear of your orthotics your symptoms, in theory at least should improve. Keep in mind, most people do not wear their orthotics all day long, so for example, if you come home at dinner time and kick off your shoes, you are then walking around for the next few hours pronated and re-aggravating your tarsal tunnel. There is also a possibility that you may be able to tolerate more support than you have in your orthotics. More support, means less nerve irritation. Let your podiatrist decide on that. Keep in mind that excess pronation is probably the most common cause of tarsal tunnel but not the only. Another cause could be a growth of some sort in the tarsal canal which will also put pressure on the nerve. I mention this because if you do not fully improve I would recommend an MRI of the tarsal tunnel canal to look for any abnormality which might explain why you still have issues. Short of that, if after a period of time wearing your orthotics still gives you only moderate relief, speak to your podiatrist about a possible cortisone injection into the tarsal tunnel canal or even a round of oral prednisone. I also think your podiatrist has to take into account any residual effects from your right hip surgery as that may be affecting your gait as well. At age 51 the arthritis in your midfoot is the result of being pronated, it is not the cause or precipitating factor in pronation. The accessory navicular may or may not be a precipitating factor in your flat feet.
Marc B. Mitnick, DPM
Visitor Name: Donna Location: Downingtown, PA, United States Question: Tarsal Tunnel Syndrome During an examination by a nurse practitioner, a member of my family practice group, she knuckled my arch which caused instant severe pain. I have been later diagnosed with having Tarsal Tunnel Syndrome. Is it possible that her examination caused this syndrome? RESPONSE Hi Donna, I doubt that knuckling your arch caused tarsal tunnel, particularly since the tarsal tunnel canal is more in the area just below the medial malleolus (the medial ankle bone) and not in your arch. There is always the possibility that the knuckling injured something directly in that area but I do not think it would be mistaken for tarsal tunnel. Key Observation: If you have tarsal tunnel syndrome, this is something that usually takes a while to develop, in many cases from the way you walk, particularly flat-footed. In a foot that flattens out too much (over pronates), that creates a jamming on the outside of the ankle and a stretching on the inside of the ankle. It is this stretching that puts pressure on the ligament over the nerves in the tarsal canal. This ligament then puts pressure on the nerves and you end up with the symptoms of tarsal tunnel. There are other situations that can cause tarsal tunnel, such as trauma itself to the tarsal canal or perhaps a growth of some sort that also puts pressure on the nerves as they pass through the canal. You do not mention if you are still having severe pain where the foot was knuckled so I do not know if that warrants any discussion. Marc Mitnick DPM
tarsal tunnel pain
tarsal tunnel test
Condition
Primary Symptoms
Distinguishing Feature
Diabetic Neuropathy
Symmetrical numbness or burning in both feet.
Related to blood sugar levels; usually affects both feet in a "stocking" pattern.
Peripheral Neuropathy
Tingling, numbness, or "pins and needles."
Can be caused by alcoholism or vitamin deficiencies rather than physical compression.
Radiculopathy
Pain radiating from the lower back down to the foot.
Symptoms follow a specific nerve path (dermatome) originating from the spine.
Plantar Fasciitis
Sharp heel pain, especially with the first steps in the morning.
Pain is localized to the bottom of the heel; usually lacks the radiating burning of TTS.
Baxter's Nerve Entrapment
Chronic heel pain mimicking plantar fasciitis.
Specifically involves the first branch of the lateral plantar nerve; often misdiagnosed as a heel spur.
Ganglion Cyst/Lipoma
Localized swelling; pain if the mass presses on the nerve.
A physical "lump" or soft tissue mass may be visible on an MRI or felt in the canal.
Vascular Disease
Aching or cramping in the feet, often worse with exercise.
Related to circulation; skin may be cool to the touch or show color changes.
HOW DO YOU TREAT TARSAL TUNNEL SYNDROME
orthotics for tarsal tunnel syndrome
Treatments include the use of orthotics when the origin of the problem appears to be excessive pronation.
tarsal tunnel exercises and home remedies
TARSAL TUNNEL RELEASE PROCEDURE
Frequently Asked Questions



Specific Recommendations For This Condition
KLM ORTHOTICS
In my opinion, the best pre-made orthotic available. Offers the best combination of support and cushioning. Will work in the greatest percentage of people who try a pre-made orthotic. (keep in mind, everyone's foot structure is different and so unlike a prescription orthotic, pre-made devices can be hit or miss). In order to treat capsulitis, this orthotic has to be ordered with a metatarsal pad. Click the link below for a full description.
![]()
Questions I have answered from visitors
Patient FAQ: Differentiating Baxter's Nerve vs. Tarsal Tunnel Syndrome
Location: Cincinnati, Ohio
If you happen to live in the New York - New Jersey area and would like to visit our office
|
|
To make an appointment online or for directions to our office click Dr. Marc Mitnick.
DISCLAIMER: The purpose of this site is purely informational in nature. It is not intended to diagnose, treat or cure any medical condition. This information is not a substitute for advice from a medical professional. Please consult your healthcare provider for accurate diagnosis and treatment. The information presented here may be subject to errors and omissions.
SITE LAST UPDATED: MAY 2026

I've been doing some aggressive research lately (it's how I found your incredible website) and realize now that my symptoms are not consistant with the diagnosis.
Jennifer
Hunterville, NC
….after reviewing your amazing site (great for the avg. jill). So thank you very much!!!
Liesbeth
NY
I am really, really impressed with your plain-speak explanations for the various conditions.
Jacqueline
NJ
This was an extremely helpful site. I have an appointment on the 18th and your info. Was right on target…..
Jack
Fla
A well organized site containing much information written in a manner that the average reader can comprehend.
Jean
Ontario, Canada
I found your website and articles most interesting.
Andrew
Fla.
Thank you for a quick response. I think your site is the best information site on foot pain and I have viewed many.
Judy
(location unknown)
I came to your website, footspecialist.net via www.foot-pain explained .com which I think is also your website? I thought explanations for different types of problems were well addressed and thoughtfully stated for the patient in mind.
L.W.
New York
You have an amazing and extremely informative site. I enjoyed looking through all of the data and stats.
Yvette
Memphis, TN
Thanks again so much for the information in the article. Very interesting.
Anna
Scotland
Great article. I have had plantar fasciitis since I was in high school……..
J. Simmons
(location unknown)
Dear Dr. Mitnick, The orthotics arrived four days ago and I slipped them into my shoes immediately. I was skeptical as to the usefulness of the item, they really didn't look very exotic. I have to say though, after using them for just four days, I have experienced grand relief from my foot pain. Even the very first day, I was able to do a lot of work while on my feet with at least a 75% reduction of pain. It has only gotten better every day, and I go nowhere without my shoes with the orthotics. I had been experiencing extreme heel and sole pain for about six months and had to take extended breaks off my feet many times a day as well as regular doses of Ibuprofen. Since getting the orthotics, my life has returned to normal and I feel good again. Just wanted to say thanks for the recommendation for a very effective item, I had no idea what a change this item could affect.
Yours truly,
J.C. Forbes
Tennessee
Thanks for the Response, you hit it on the head.
Steve
Redondo Beach, CA
Thank you for your time and expertise in answering my question…..
LH
(location unknown)
First, thanks for putting together this website. Its the most informative site I have found dealing with foot problems. Last June I started having pain and swelling at …….
Joe
(location unknown)
First of all, thank you for having all this useful information available in one place. I've been through most of your website and based on my research, pain and evaluations I think I've narrowed things down quite a bit.
Pete M.
(location unknown)
Thank you for the best site I have found when researching foot pain.
Glenda B.
Madison, Alabama
Thanks for replying so quickly. I was a bit concerned. I think your website is great, and chock full of info.....
Carol
Denison, TX
Dr. Marc, Thank you so much for your reply which seemed to be right on. I have researched many sites but you put me on the right path to the possible answer. My foot pain may not rule the rest of my life after all! I believe I'll make a sign that reads, "THE END IS NEAR!" Thanks Very Much,
Dawn
West lafayette, IN
Dear sir...no doubt you get positive comments re your site...May I please be added to the list of your admirers. In all of my years of web surfing I would say your site is right there with the very best. Thank you for taking the time to write the terrific info you provide and for putting things into laymen terms for us mere mortals. I pray you have much on going success and thank you again for a deed well done. As for me I did not find much help for my symptoms and will continue on my quest. Were you anywhere in the South I would make and appointment...Thanks again dear sir...m.e.
Michael E.
Tampa, Florida 33624
Hi. This is a great site! I'm a healthy middle aged woman who is in good health, but.....
Kelly
Texas
Just a wee word of thanks for your wonderful website...It is a terrific service...Thank you for providing your knowledge and help...With highest regards, m ebeling
Michael D. Ebeling
Tampa, Florida 33624
Thanks for a most interesting website, which has helped a lot.
Steve
UK
Dear Dr.Mitnick
I usually do my research on the Mayo clinic website. I think your website is the most informative site I have found when researching foot pain.
I thank you for putting together this incredible website.
Regards,
Dragica W.
Edmonton,Canada
....I have been told that it is not hard enough to be cut off. Please help, I am not sure what to do now! THANKS FOR A WONDERFUL AND VERY HELPFUL SITE!
Roxy
South Africa
You have an unusually clear, informative and well-written website for laypersons. Thank you for that.
Matthew W.
Mansfield Ctr, CT
First, I'd like to thank you for all the information that you provide on your website and the opportunity to write to you.
Steve
Placentia, California
First, I want to let you know that you have the best web site I've found related to foot issues. (The only thing I had difficulty finding was the "ask a question" page.)
Unknown
Unknown location
I received the orthotics Monday afternoon and began wearing them Tuesday. After two days I would say that I have noticed a huge improvement in the discomfort I have been experiencing. My foot feels better than it has in months.
Ric J.
Unknown location
I greatly admire someone like you who would donate and dedicate so much time and effort to helping strangers with no compensation. Truly, it is uncommonly kind. And your site is so intelligently arranged.
Ron R.
Pacific Grove, CA
I used to work for a podiatrist (front desk) back during summers in college years ago, so I know the benefits of good care. Again, I want to thank you for an EXCELLENT website. It was so great to get to your site (top of google search) and actually find all the answers I needed EASILY and QUICKLY! Clearly you put a ton of work into it and I really appreciate it.
All the best,
Victoria
Alameda, California
By the way, millions of websites could use yours as a guideline on how to organize information and make the site user-friendly. Kudos to you!
Anonymous
Thank you for your very interesting and informative site!
Anonymous
Hi. I come to your site often looking for information. It is really informative and I appreciate it very much. I have RA and have been having considerable amount of foot pain...... Dee RN
Thanks very much for the wonderful informative site.
Catherine
New Zealand
Thank You for my answer! I have been schedule for a bone density scan, allingment, and I am in the process of getting orthotics made, and checking out the natural remedies. Thank again! What a great web site!
Sincerely
Josette
Yes I want both pair of orthotics. You don't have an option of ordering 2 at one time so I had to place the order twice. Thanks. My husband likes these and wants to put them in all of his shoes. (referring to Superstep orthotics)
Cindy H.
Arizona
I searched the internet everywhere for a clear description and illustration of my symptoms/problem. https://www.foot-pain-explained.com/ was where I ended my search with answers. If I lived in Jersey (left 30 years ago) and didn't live in Florida I would definetly make an appointment with Dr. Mitnick.
Thanks, Kathy
Florida
1st of all THANKS A LOT for your great site......
Anna
Poland
Thank you so much for your response. I will let you know how I am doing if you would like. Your website is awesome!
M P
South Carolina
Hello! I want to thank you for such an informative website! I found you based on my ankle pain search and am happy to realize that there may be a relatively simple cause and solution....
Natalie
unknown location
...Thanks for your fantastic service.
Gary
Arlington, VA
Thank you so very much, that would be much appreciated. I love those insoles, by the way. (referring to Superstep orthotics)
Kelly W.
San Clemente, CA
Dr Marc is fantastic...He seems to know exactly what you are feeling with the problems you are having. I wish he was in my home town so I could go to him with my problems!!!!!!!!!!!!!
Pam
location unknown
Great insights! Thanks Doc, you're the best.
Glen
location unknown
I have been experiencing foot pain of various sorts and am working to figure out what it is. I found this site and can only say BRAVO!! What an excellent site! The time it must have taken to put all this together must've been a daunting task! I am sure it has helped so many people. Thank you so very much for doing this.
Bre
location unknown
Dr. Mitnick, Thank you so much for your reply. I did let my physician know and they took an x-ray - all is well! Also, thank you for providing this wonderful site, it is very helpful with lots of useful information! I appreciate your gift of time! God bless.
anonymous
Dr. Mitnick, Thank you, you were 100% correct. The pain finally brought me to the ER. I spent 8 days in the hospital. The Doppler you spoke of was able to show that there was no pulse in that foot. This was an arterial clot that split and traveled throughout my leg. My leg was almost amputated. I am in rough shape but have all my parts intact!! You certainly know what you are talking about. Thank you for taking the time to answer. Yours Truly!
anonymous
Staying at home after hallux surgery I spend quite a lot of time seaching info useful for avoiding problems which might come back. Today I found your site and I am .... delighted it happened. It's one of the best site I found last days.
Anna
Poland
Thanks for taking time to read and answer so many questions. It is truly a public service!
Esh
Seattle, WA
I just wanted to say that I am very greatful for this website!!
Bonnie
location unknown
Also, and importantly, just want to praise this web site. Thorough and thoughtfully presented, it certainly must be of considerable assistance to anyone with a foot problem. Terrific -- and very interesting.I trust the address comes up easily for those seeking information.
Bill
New Jersey
Thanks so much for answering my question. You've been more help to me than my own Dr. has been lately. Thanks again....I hope to be able to walk without pain someday.
Debbie
location unknown
Wow, that is exactly the information needed!!! thank you thank you thank you!!! I appreciate this help so very much from Marc Mitnick DPM. Excellent information and help to improve One's life.
Chrissy
location unknown
Thanks so much for this website Dr. Marc! It is so nice that you have this ask the doctor feature..I'm sure I'ts been helpful for alot of people. I will try what you suggested and see if it helps...thanks again!
Tracy
Evansville, IA
Dear Marc
I just want to say thank you for the quick response and the good info. I find it amazing and a super nice thing that you do here by answering medical questions at no charge.
Russ W.
location unknown
Your website is full of a lot of helpful information, and I am very impressed with the time in which you responded to my post. Thank you again for your time and consideration in your response.
-Sunny.
location unknown
Thank you very much for the information, I will consider it. Excellent web site.
Jackie
San Diego, CA
Dr. Mitnick, Just want to say thank you so very much for your quick response and very informative reply! After reading what you had to say, I called the doctor's office and was able to get in and see him the same day as my injury. Toe was x-rayed and luckily, it is not broken or fractured. Very badly bruised and will probably lose the toe nail. And although my toe and toe nail are still very black and blue and very sore, they ARE both starting to feel a little better. So again, thank you! I am so very happy that I came across your website. The service you provide is outstanding and immeasurable!
Rivi,
Albany, NY
Thank you so much for all of your advice. In searching the web for people dealing with this same issue i can tell you that you are a Knight In shining Armor! If I lived in Jersey I would gladly be your Spokesperson. Hopefully next time you hear from me it will be good news. God Bless,
Jill S.
location unknown
THANK YOU SO VERY MUCH FOR YOUR TIME AND EFFORTS, YOU ARE SO VERY APPRECIATED. THANK YOU FOR ALL YOU DO.
Jackie
Whichita, KS
thanks again, this site is very helpful.
mark
Boston, MA
Like others have stated...This site is amazing and I am so thankful that it was created.
....Keep up what your doing. Your a life saver.
Michelle
Colorado
Thanks again for the information provided on your site. It's easy for non-medical folk to understand your writing, and helps provide better communication between patient and doctor.
annielou
Colorado
Wonderful advice
by: Anonymous
This is the best site for foot problem info.
Thank you for this information. This description fits my pain and inflammation behind my 2nd toe perfectly.
by: Max
location unknown
Again, I really appreciate that you responded to my inquiry, and that your mention of Parkinson's helped me to find my way to a diagnosis of this difficult to diagnose disease. Most patients see on average 16 doctors before they are diagnosed. I hope that you can help other people that ask for your expertise in the future.
Barb D.
Canada
I just wanted to say that I am very greatful for this website!! I have had a fusion in my rt foot and am finally getting a little bit better......
Bonnie
location unknown
Again, Thank you from the bottom of my heart for taking the time to answer my question....your an angel!
Nancie
Wisconsin
Thank you for your response. You have provided some great insight (to my question)....
Julie
location unknown
Thank-you so very much for responding so quickly and in such detail to my question!! I will give my surgeon a call today!! This website is terrific!!!! Thank-you again!
Renae
North Carolina
Many Thanks Dr Marc!
Thank you for your response. It sounds like a good plan to me. He did not cut the wart out first ...
KG
location unknown
Thanks again doc for having this website and we STILL need qualified Podiatrists in beautiful sunny Tampa Bay (Bradenton) Florida.
Bessie Mae
Florida
Dear Dr. Mitnick, Thank you so very much for taking your time to answer my question. You have greatly relieved my anxiety related to the continual tingly I feel in my feet. I will share your response with my podiatrist next week. God bless you for having this question and answer page on your website! Most gratefully,
Lynne T.
location unknown
Your webpage is excellent, I commend you on sharing your knowledge to the public.
Robert
New Jersey
Thank you. you were more detailed than what others have told me they finally called from the last xrays and my son is now in a cast for 2 weeks he did have a fracture that was not noticeable.
a mom
location unknown
I have read your website and I have to admit that I am amazed at all the information that is on here. I have learned more than the three years I have been going to several doctors that I have seen!!
Melody
Lenoir, NC
Thank you so much Doc for a quick and thorough response!
Rustam
Bellevue, WA
I cannot thank you enough for your response, opinion, and suggestions! I want you to know how much it means to me, and I'm sure everyone else who has ever asked you a question! I feel like you're a lifesaver and have empowered me to take a stronger role and stand up for myself and my feet!
Jodi
location unknown
Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…