- Home
- circulation
peripheral circulation
Peripheral arterial and venous circulation play a critical role in the health of the feet, and impairment in either system can lead to pain, tissue damage, ulceration, or even gangrene. As circulation declines with age, factors such as diabetes, smoking, hypertension, and lifestyle habits greatly influence how well blood reaches—and returns from—the feet.
Arterial disease most commonly results from atherosclerosis, where fatty deposits and thickening of the artery walls restrict blood flow. Early signs include calf pain after walking (intermittent claudication), temperature differences between feet, color changes, and non‑healing sores. In advanced cases, the skin may appear thin, pale, shiny, and may develop ulcers or gangrene, requiring interventions such as angioplasty, stenting, or bypass surgery.
Venous insufficiency, by contrast, involves poor return flow from the feet back to the heart. This often presents as swelling that worsens throughout the day, aching, heaviness, itching, or visible varicose veins. Severe cases may progress to venous stasis dermatitis or ulceration. Treatment ranges from compression stockings to sclerotherapy or surgical vein removal.
Circulatory disorders can also appear in younger individuals due to overuse injuries, anatomical abnormalities, or rare inflammatory conditions such as Buerger’s disease. Proper diagnosis typically requires vascular testing, including Doppler studies, ultrasound, or advanced imaging.
Early recognition of circulation problems is essential. Symptoms such as rest pain, color changes, persistent swelling, or non‑healing sores should prompt evaluation, as timely treatment can prevent serious complications and preserve limb health.
Reviewed by: Medical Review Board
ARTERIAL CIRCULATION INTO THE FEET
When we as foot specialists examine a foot, we break it down into four systems: dermatological, orthopedic, neurological and vascular. The vascular or circulation system is further broken down into arterial blood flow into the foot and venous which is blood flow away from the foot back to the heart.
Of the four systems, peripheral circulation problems are potentially the most damaging to the foot. Lets face it, without proper blood flow to the foot or impaired circulation away from the foot the tissues of the foot will suffer and in some cases die (gangrene).
Unfortunately, as we age our peripheral circulation to our feet does become impaired. The degree of impairment will vary from person to person with factors such as genetics, life style (smoking, poor diet, lack of exercise), and other disease states (diabetes, hypertension,) all contributing to a decreased blood flow to and from the foot.
When the foot is examined in regards to peripheral circulation we note the following:
- ability to feel pulses and the strength of those pulses
- color and texture of the skin
- hair distribution as loss of hair can but not always signal a loss of circulation to the foot
- rashes
- ulcers
- venous patterns and venous enlargement
- edema (swelling)
- temperature decreases
- temperature differences between the two feet. In general, one cold foot is suggestive of poor circulation, two cold feet may be indicative of anxiety, neurological or a cold environment.
patient complaints that may suggest poor peripheral circulation
- A change in a patient’s recent history can give us a clue to circulatory impairment. If a patient complains of rest pain meaning their feet and legs will hurt at night, but find that if they put their feet in a dependant position (sitting), or even standing, the pain subsides that is highly suggestive of circulatory problems.
- People who complain of walking a few blocks and experiencing calf pain, finding that if they stop and rest the pain goes away, only to return when they walk about the same distance is highly suggestive of vascular problems.
- Changes in color of the feet when in a dependent position compared to when the feet are elevated.
- Sores on the feet that do not seem to heal is a normal period of time.
- Feet and ankles that appear normal in the morning but progressively swell during the course of the day may be exhibiting poor venous flow. Keep in mind that there is varying degrees of swelling and not all swelling is indicative of serious disease, however, on the other hand if one foot is constantly swollen then circulatory compromise has to be ruled out.
what is atherosclerosis
The most common cause of poor blood flow into the foot is atherosclerosis or hardening of the arteries. This is a progressive degenerative process characterized by the deposition of fatty substances inside the wall of the artery along with a fibrous thickening of the artery wall resulting in a diminished ability of blood to flow down to the foot.
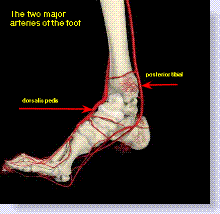
Below is a diagram of the arterial flow into the foot.
|
This condition in most people will go undiagnosed until the condition becomes symptomatic. When the initial symptoms of intermittent claudication (pain in the calf after walking a short distance, although to a lesser extent the thighs and buttocks) presents, there is already significant disease present.
What is essentially happening, due to blockages in the blood flow to the feet, there is a mismatch between the oxygen supply being supplied to the extremities and the metabolic demands of the muscles of the feet and lower legs upon exertion. Simply stated, when muscles are working, they need fresh oxygen to supply them. Any reduction in this oxygen supply to a muscle will cause pain (claudication).
This condition occurs predominately among men between the ages of 50 and 70 years and usually starts after age 60 in women. Race and ethnic background also play a role as African Americans have a higher incidence of peripheral arterial disease (PAD) than non-African Americans. Studies have also shown that Hispanics present with more advanced lower extremity vascular disease and have worse outcomes, which includes a higher amputation rate after revascularization, than non-Hispanic whites. (Lower Extremity Review, March 2013). An estimated 8-12 million Americans have this condition. Fifty percent of people with PAD (peripheral arterial disease) are asymptomatic and usually go undiagnosed.
Major causes of atherosclerosis include:
- diabetes, which affects both the major blood vessels bringing blood into the foot and the smaller vessels, which actually supply each area of the foot.
- Hypertension or high blood pressure can also cause damage to the arteries of the foot and leg and over time diminish blood flow to the feet. It is also worth mentioning that some anti-hypertensive medicine will also adversely affect the feet in that they can cause swelling and discoloration of the extremities.
- Smoking, however, may be the worst cause of damage to the arteries that bring blood to the feet (as well as the heart, brain and kidneys). Smoke from tobacco directly damages the inside of the arteries.
Here is a summary of conditions that may lead to atherosclerosis:
| Condition / Factor | Impact on Arteries | Primary Risk Level |
|---|---|---|
| Smoking | Directly damages the internal lining of the arteries; causes chemical injury to the vessel walls. | High |
| Diabetes | Affects both large major blood vessels and smaller "micro" vessels supplying specific foot tissues. | High |
| Hypertension | Creates chronic strain and damage to the artery walls, diminishing overall blood flow over time. | Moderate / High |
| Genetics & Lifestyle | Poor diet and lack of exercise contribute to the deposition of fatty substances and plaque. | Variable |
| Overuse Injuries | External damage or "fibrotic bands" can impinge on blood flow (more common in younger patients). | Low (Specific cases) |
Abnormal causes of atherosclerosis
Although atherosclerosis is generally associated with middle age and elderly individuals, there are instances where young people are affected.
A 17 year-old Irish dancer developed discomfort in her toes as well as discoloration and swelling over a one year period. She was an otherwise healthy individual, not taking any medication. An MRA (magnetic image angiogram) was performed and revealed fibrotic bands of the dorsalis pedis artery which is the artery on top of the foot that runs from the ankle all the way down to the toes.
An ultrasound was then performed that found the fibrous bands were impinging flow of blood through the dorsalis pedis artery when the foot was plantarflexed (pointed downward). Essentially her circulation was being cut off.
Surgery was performed to resect the bands and bounding pulses returned to her feet.
The lesson learned here is that even young people can develop vascular compromise. The majority of these cases are usually from external damage to the arteries through overuse injuries.1
treatment of atherosclerosis
There are a few different treatments for arteriosclerosis in the lower extremity and treatment is based on a number of factors including the degree of blockage either by occlusion (calcified plaque) or by stenosis (narrowing of the artery), the age of the patient, their general overall health, etc.
- As of this writing (April,2008) walking is considered the primary treatment in treating arteriosclerosis in mild to moderate cases. In fact walking works better than oral medication. However, we are talking about a daily walking program on a graded treadmill for 30 minutes. Initially, that may be impossible for many, so you need to work up to that number. This should be a supervised program and you should have clearance from you doctor. Exercise on a regimented, physician supervised program can reduce the symptoms of intermittent claudication in as little as 6 months in many individuals. The problem here is that many people would rather pop a pill daily than to go out and get some exercise, but statistically it has been shown that walking is far superior to medication in this situation. (Vascular Medicine and Intervention2, Holy Name Hospital Interventional Institute, April 2008).
- Medications used for peripheral arterial disease include Cilostazol which increases blood flow by dilating (opening up) arteries and Pentoxifylline which works by making red blood cells more pliable so they can "squeeze" through narrow arteries.
Below is a picture of very poor circulation into the foot. Notice how pale, thin and shiny the skin is along with sores that have developed on the foot.

- Once a foot has reached this state exercise or medication is no longer going to cure the problem. Either an angioplasty, stent or bypass surgery will be required to bring the foot "back to life". The image below reveals gangrene of the toes which eventually lead to amputation.

|
VENOUS CIRCULATION OUT OF THE FEET
The most common cause of poor blood flow out of the foot is varicose veins. This is a very common disorder seen twice as often in women than men and the prevalence increases with age.
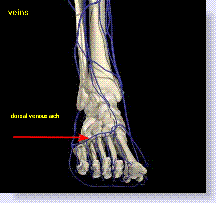
Below is a diagram of the venous system in the foot.
|
symptoms of venous insufficiency (poor venous flow)
- Generally, the patient’s foot and ankle will be normal in appearance in the morning only to swell as the day progresses and return to normal the next morning.
- The common complaint is a feeling of a dull heavy ache that develops after long periods of standing, which is relieved by elevating the leg or by the use of elastic stockings.
- Occasionally symptoms of itching, burning and cramps may also be present.
Increased humidity, obesity and the cyclic premenstrual period may exacerbate the symptoms.
treatment of venous insufficiency
- In simple to moderate cases, compression stockings may relieve the symptoms. They should be applied first thing in the morning before the extremity has started to swell, however in those that require a heavier compression, the stockings can be very difficult to put on and take off and can be very uncomfortable in hot weather.
- Injection of saline and other chemicals may be used to force the veins to collapse, which in itself may not improve return circulation but will make the protruding veins more cosmetically acceptable. This is known as sclerotherapy.
- Surgical "stripping" or removal of the offending varicosed vein.
- Under the category of "folk remedies" there are two ways to minimize simple varicose veins.
The first is apple cider vinegar. Soak a cheesecloth bandage in apple cider vinegar and use it to wrap the affected area for thirty minutes. Make sure you legs are reclined above the level of your heart. Do this twice a day. Vinegar is believed to encourage varicose veins to contract. Some people also suggest drinking two teaspoons of apple cider vinegar in a cup of warm water after each session.
The second is bromelain. This collection of enzymes found in pineapples has anti-inflammatory properties believed to inhibit the unattractive swelling around varicose veins. Take 500-1000mg with each meal. Bromelain is available in health food stores.
WORSENING OF VENOUS INSUFFICIENCY
In more severe cases of venous insufficiency the leg can become chronically swollen and inflamed. The leg is now much more susceptible to ulceration and infection.
Below is a picture of severe venous stasis. Notice the swelling and discoloration of the leg. A complication of this condition is a venous stasis ulcer.

|
Deep venous thrombosis is also a medical emergency. This is a blood clot that has occurred in a vein in the leg. The classic example is severe tenderness in the calf upon pressing the area with the foot simultaneously being dorsiflexed (foot bent upward); this is known as Homan's sign.
Other symptoms include persistent or unexplained swelling usually in only one lower leg. Additionally, the leg may also be red in color. This should not be confused with intermittent claudication, which generally results in calf pain after walking and no swelling in the foot and ankle.
The diagnosis is usually made with the use of a venogram, and more recently with duplex venous ultrasound. In patients who exhibit shortness of breath, fever, rapid heart beat or dizziness, a pulmonary embolism also has to be ruled out.
Factors that increase the chance of a deep venous thromobus (DVT) consist of:
- injury to the inner wall of the vein
- a hypercoagulable state which means means the blood has a greater tendency to clot. Factors such as smoking, malignancy, use of birth control pills, hormone replacement therapy, congestive heart disease and obesity all can contribute to this problem.
- people who exhibit venous stasis or excessive pooling of blood in the veins around the lower leg are also more prone to forming a DVT. The most common risk factor, however, is a previous history of embolism in the lower extremity.
People with any of the above mentioned conditions which may lead to a DVT should be very careful when contemplating foot or ankle surgery and should make their doctor aware of any of the above problems. Hopefully your surgeon will take a proper history and these problems will become known during the interview.
Most cases of DVT following lower extremity surgery is associated with major orthopedic procedures involving the hip and knee but a blood clot can form after foot and ankle surgery so it is imperative both patient and doctor are aware of the possibility.
Below is a picture of DVT, deep venous thrombosis of the right leg.

|
This condition requires hospitalization and anticoagulant medication to break up the clot. Without treatment there is a very high incidence of the clot breaking loose and causing a pulmonary embolism, which is a life-threatening situation. This type of clot is also known as (VTE) or venous thromboembolism.
A more common condition with less potential complications is a superficial phlebitis. This is an inflammation of one of the superficial veins such as on top of your foot that forms a clot and inflammation ensues.
This is usually a benign and self-limiting condition. Typically, a patient will present complaining of a painful, red area on the foot or lower leg with a lump underneath the skin. The lump is cord-like in its appearance. They can occur spontaneously or after trauma directly to the area.
Treatment consists of warm compresses and anti-inflammatory medication.
NOTE: there are many more conditions of peripheral circulation that have not been discussed. For example, see my discussion on blue toe syndrome.
Buerger's disease
One vascular problem affecting both the arteries and veins that I would like to mention is a condition known as Buerger's disease or thromboangitis obliterans. I have seen one such case and that was during my residency, but found it to be fascinating.
Buerger's disease is a condition that affects medium sized arteries and veins leading to the hands and feet. It is an inflammation of either the arteries or veins which thus causes a blockage of blood flow usually into the fingers and toes. It is a condition that has a predominance in jewish and asian populations affecting men three times as much as women. The incidence in the United States is estimated to be 12-20 cases per 100,000 population. The disease is most prevalent during the ages of 25-40 years.
No immunologic or toxic basis has been identified as the cause of this condition, but there is a very strong correlation with tobacco use. Tobacco itself has the propensity to thicken the inner lining of blood vessels as well as cause vasoconstriction (clamping down) on vessels further diminishing blood flow.
Thromboangitis obliterans has two stages:
Early Stage- where there is periodic episodes of inflammatory reactions which essentially inflame the internal lining of arteries and veins causing a diminished flow of blood into the fingers and toes and obstruction of veins by thrombosis which does not allow for proper blood flow from the fingers and toes back to the heart.
Late Stage- constriction of arterial flow to the point where ulceration and possibly gangrene set in at the ends of the fingers and toes. Thrombophlebitis of the venous system resulting in medical emergency as well as formation of ulcers along the course of the veins.
Diagnosis is made by taking a thorough history with any admissions of tobacco use. Once this condition is suspected, it can be confirmed through a multitude of vascular testing. This includes doppler studies of the arteries as well as plethysmography which measure blood volume in the fingers and toes. Ultrasound studies measuring venous flow are also performed, as well as nuclear imaging.
Treatment options for Buerger's disease include cessation of smoking, although in the one case I have observed, the patient continued to smoke even as his toes were being amputated one by one. Anticoagulants may be used for any thrombophlebitis that may develop. Anti-inflammatory medication is also used in sub-acute incidences of phlebitis. Vasodilators which attempt to open up vessels for increased blood flow are used in early stages to reduce the vasospastic component of the condition. Lastly, in many cases amputation is necessary if any ulceration becomes grossly infected or if gangrene has set in.
The more serious conditions described above are generally diagnosed with sophisticated testing such as arteriograms and venograms along with dopplers and nuclear imaging. Inspecting the area can give us an idea of the problem but testing confirms them. These conditions are best diagnosed and treated by vascular surgeons, however, the local treatment of any foot manifestation is usually best in the hands of a podiatrist.
Cutting Edge NewsOver the last year or so, the pomegranate has been the subject of a lot of research in health as a potent antioxidant. An article from the Life Extension Foundation discusses recent research revealing
how not only does pomegranate slow down atherosclerosis but it actually may reverse it.
To read the entire article, click
here |
1 Foot Claudication with Plantar Flexion as a Result of Dorsalis Pedis Artery Impingement in an Irish DancerSmith BK, Engelbert T, Turnipseed WD, (University of Wisconsin Hospital and Clinics, Madison, WI)
J Vasc Surg 2013 Jul;58(1):212-214
ADDITIONAL REFERENCES
Frequently Asked Questions
Questions I Have Answered From Visitors
Question: Blue and Purple Discoloration Post-Partum
Hello and thank you in advance for taking the time to listen. I am going to try and be as specific and brief as possible. This is for my wife, whose feet have been extremely blue and purple around the sides of and on the bottoms of her feet. Her toes are also purple all over even underneath her nail beds. We have been to our PCP, a vascular surgeon and even the ER. No one as of yet has been able to give us a definitive answer.
We discovered the discoloration 5 days ago and at the time, there was no pain involved. On the third night, the pinky toe on her left foot started causing her minor pain. Since then, that same toe has become excruciatingly painful to the point where 1000mg of Vicodin barely helps. The pain is intermittent and occurs up to 2 times/hour and lasts up to 4-7 minutes.
Background: My wife is 28 years old, 2 and 1/2 months post-partum with our first child. She spiked a fever during labor and was given antibiotics, other than that there were no other complications. 2 weeks ago she was diagnosed with ulcerative colitis and was prescribed 3600 mg of Asacol daily. She took this medication for a week and a half but it seemed to make her feel worse. She stopped taking the Asacol and the problems with her feet started 2 days later. She went back for a check up and they discovered her WBC count hasn't gone down and her potassium was low. They also found a UTI and prescribed Ciproflaxin and Potassium CL.
Our most recent trip to the ER yielded almost no results. A vascular surgeon says we may have vasculitis and a nurse suggested Raynaud's phenomenon. The surgeon prescribed Nifedipine, a calcium blocker. They simply took her pulses and said everything was okay. My wife and I are very worried since there has been no real diagnosis and the pain becomes more frequent. The color really bothers me, but the doctors say the color doesn't bother them, only the pain. According to them, the pulses are good and the feet are blanching, so circulation is fine. My wife is scared of losing her toe; it breaks my heart to see her in so much pain.
Dr. Mitnick's Response
Hi Brian,
Discoloration like you describe is NOT normal, particularly if it never existed before, and especially in a 28-year-old woman. Just because you can palpate her pulses doesn't tell the whole story; there may be an issue with the blood returning to her heart.
I find this particularly troubling because she just gave birth. My first thought would be a blockage of some sort at the level of her pelvis, preventing blood from returning to the heart; this would discolor her feet. In addition, she may have thrown a small embolism which will discolor her feet, but not always block the blood flow into her feet entirely—which is why the vascular surgeon still felt pulses.
This discoloration may have also been a result of some of the medication she was on; while I am not familiar with every specific reaction for all of those, certain medications can cause discoloration in the feet.
This is just some things that come to mind without having the luxury of being able to visually examine your wife's feet. Have you discussed this with her obstetrician? If not, a phone call to that office might shed some light on the problem, or at least rule out her pregnancy as being the source of the problem.
Also, do not use heat in an effort to warm up her feet; if she is suffering from a circulatory disorder, you are only going to make it worse.
Marc Mitnick DPMIf you happen to live in the New York - New Jersey area and would like to visit our office
|
|
To make an appointment online or for directions to our office click Dr. Marc Mitnick.
DISCLAIMER: The purpose of this site is purely informational in nature. It is not intended to diagnose, treat or cure any medical condition. This information is not a substitute for advice from a medical professional. Please consult your healthcare provider for accurate diagnosis and treatment. The information presented here may be subject to errors and omissions.
SITE LAST UPDATED: MAY 2026

I've been doing some aggressive research lately (it's how I found your incredible website) and realize now that my symptoms are not consistant with the diagnosis.
Jennifer
Hunterville, NC
….after reviewing your amazing site (great for the avg. jill). So thank you very much!!!
Liesbeth
NY
I am really, really impressed with your plain-speak explanations for the various conditions.
Jacqueline
NJ
This was an extremely helpful site. I have an appointment on the 18th and your info. Was right on target…..
Jack
Fla
A well organized site containing much information written in a manner that the average reader can comprehend.
Jean
Ontario, Canada
I found your website and articles most interesting.
Andrew
Fla.
Thank you for a quick response. I think your site is the best information site on foot pain and I have viewed many.
Judy
(location unknown)
I came to your website, footspecialist.net via www.foot-pain explained .com which I think is also your website? I thought explanations for different types of problems were well addressed and thoughtfully stated for the patient in mind.
L.W.
New York
You have an amazing and extremely informative site. I enjoyed looking through all of the data and stats.
Yvette
Memphis, TN
Thanks again so much for the information in the article. Very interesting.
Anna
Scotland
Great article. I have had plantar fasciitis since I was in high school……..
J. Simmons
(location unknown)
Dear Dr. Mitnick, The orthotics arrived four days ago and I slipped them into my shoes immediately. I was skeptical as to the usefulness of the item, they really didn't look very exotic. I have to say though, after using them for just four days, I have experienced grand relief from my foot pain. Even the very first day, I was able to do a lot of work while on my feet with at least a 75% reduction of pain. It has only gotten better every day, and I go nowhere without my shoes with the orthotics. I had been experiencing extreme heel and sole pain for about six months and had to take extended breaks off my feet many times a day as well as regular doses of Ibuprofen. Since getting the orthotics, my life has returned to normal and I feel good again. Just wanted to say thanks for the recommendation for a very effective item, I had no idea what a change this item could affect.
Yours truly,
J.C. Forbes
Tennessee
Thanks for the Response, you hit it on the head.
Steve
Redondo Beach, CA
Thank you for your time and expertise in answering my question…..
LH
(location unknown)
First, thanks for putting together this website. Its the most informative site I have found dealing with foot problems. Last June I started having pain and swelling at …….
Joe
(location unknown)
First of all, thank you for having all this useful information available in one place. I've been through most of your website and based on my research, pain and evaluations I think I've narrowed things down quite a bit.
Pete M.
(location unknown)
Thank you for the best site I have found when researching foot pain.
Glenda B.
Madison, Alabama
Thanks for replying so quickly. I was a bit concerned. I think your website is great, and chock full of info.....
Carol
Denison, TX
Dr. Marc, Thank you so much for your reply which seemed to be right on. I have researched many sites but you put me on the right path to the possible answer. My foot pain may not rule the rest of my life after all! I believe I'll make a sign that reads, "THE END IS NEAR!" Thanks Very Much,
Dawn
West lafayette, IN
Dear sir...no doubt you get positive comments re your site...May I please be added to the list of your admirers. In all of my years of web surfing I would say your site is right there with the very best. Thank you for taking the time to write the terrific info you provide and for putting things into laymen terms for us mere mortals. I pray you have much on going success and thank you again for a deed well done. As for me I did not find much help for my symptoms and will continue on my quest. Were you anywhere in the South I would make and appointment...Thanks again dear sir...m.e.
Michael E.
Tampa, Florida 33624
Hi. This is a great site! I'm a healthy middle aged woman who is in good health, but.....
Kelly
Texas
Just a wee word of thanks for your wonderful website...It is a terrific service...Thank you for providing your knowledge and help...With highest regards, m ebeling
Michael D. Ebeling
Tampa, Florida 33624
Thanks for a most interesting website, which has helped a lot.
Steve
UK
Dear Dr.Mitnick
I usually do my research on the Mayo clinic website. I think your website is the most informative site I have found when researching foot pain.
I thank you for putting together this incredible website.
Regards,
Dragica W.
Edmonton,Canada
....I have been told that it is not hard enough to be cut off. Please help, I am not sure what to do now! THANKS FOR A WONDERFUL AND VERY HELPFUL SITE!
Roxy
South Africa
You have an unusually clear, informative and well-written website for laypersons. Thank you for that.
Matthew W.
Mansfield Ctr, CT
First, I'd like to thank you for all the information that you provide on your website and the opportunity to write to you.
Steve
Placentia, California
First, I want to let you know that you have the best web site I've found related to foot issues. (The only thing I had difficulty finding was the "ask a question" page.)
Unknown
Unknown location
I received the orthotics Monday afternoon and began wearing them Tuesday. After two days I would say that I have noticed a huge improvement in the discomfort I have been experiencing. My foot feels better than it has in months.
Ric J.
Unknown location
I greatly admire someone like you who would donate and dedicate so much time and effort to helping strangers with no compensation. Truly, it is uncommonly kind. And your site is so intelligently arranged.
Ron R.
Pacific Grove, CA
I used to work for a podiatrist (front desk) back during summers in college years ago, so I know the benefits of good care. Again, I want to thank you for an EXCELLENT website. It was so great to get to your site (top of google search) and actually find all the answers I needed EASILY and QUICKLY! Clearly you put a ton of work into it and I really appreciate it.
All the best,
Victoria
Alameda, California
By the way, millions of websites could use yours as a guideline on how to organize information and make the site user-friendly. Kudos to you!
Anonymous
Thank you for your very interesting and informative site!
Anonymous
Hi. I come to your site often looking for information. It is really informative and I appreciate it very much. I have RA and have been having considerable amount of foot pain...... Dee RN
Thanks very much for the wonderful informative site.
Catherine
New Zealand
Thank You for my answer! I have been schedule for a bone density scan, allingment, and I am in the process of getting orthotics made, and checking out the natural remedies. Thank again! What a great web site!
Sincerely
Josette
Yes I want both pair of orthotics. You don't have an option of ordering 2 at one time so I had to place the order twice. Thanks. My husband likes these and wants to put them in all of his shoes. (referring to Superstep orthotics)
Cindy H.
Arizona
I searched the internet everywhere for a clear description and illustration of my symptoms/problem. https://www.foot-pain-explained.com/ was where I ended my search with answers. If I lived in Jersey (left 30 years ago) and didn't live in Florida I would definetly make an appointment with Dr. Mitnick.
Thanks, Kathy
Florida
1st of all THANKS A LOT for your great site......
Anna
Poland
Thank you so much for your response. I will let you know how I am doing if you would like. Your website is awesome!
M P
South Carolina
Hello! I want to thank you for such an informative website! I found you based on my ankle pain search and am happy to realize that there may be a relatively simple cause and solution....
Natalie
unknown location
...Thanks for your fantastic service.
Gary
Arlington, VA
Thank you so very much, that would be much appreciated. I love those insoles, by the way. (referring to Superstep orthotics)
Kelly W.
San Clemente, CA
Dr Marc is fantastic...He seems to know exactly what you are feeling with the problems you are having. I wish he was in my home town so I could go to him with my problems!!!!!!!!!!!!!
Pam
location unknown
Great insights! Thanks Doc, you're the best.
Glen
location unknown
I have been experiencing foot pain of various sorts and am working to figure out what it is. I found this site and can only say BRAVO!! What an excellent site! The time it must have taken to put all this together must've been a daunting task! I am sure it has helped so many people. Thank you so very much for doing this.
Bre
location unknown
Dr. Mitnick, Thank you so much for your reply. I did let my physician know and they took an x-ray - all is well! Also, thank you for providing this wonderful site, it is very helpful with lots of useful information! I appreciate your gift of time! God bless.
anonymous
Dr. Mitnick, Thank you, you were 100% correct. The pain finally brought me to the ER. I spent 8 days in the hospital. The Doppler you spoke of was able to show that there was no pulse in that foot. This was an arterial clot that split and traveled throughout my leg. My leg was almost amputated. I am in rough shape but have all my parts intact!! You certainly know what you are talking about. Thank you for taking the time to answer. Yours Truly!
anonymous
Staying at home after hallux surgery I spend quite a lot of time seaching info useful for avoiding problems which might come back. Today I found your site and I am .... delighted it happened. It's one of the best site I found last days.
Anna
Poland
Thanks for taking time to read and answer so many questions. It is truly a public service!
Esh
Seattle, WA
I just wanted to say that I am very greatful for this website!!
Bonnie
location unknown
Also, and importantly, just want to praise this web site. Thorough and thoughtfully presented, it certainly must be of considerable assistance to anyone with a foot problem. Terrific -- and very interesting.I trust the address comes up easily for those seeking information.
Bill
New Jersey
Thanks so much for answering my question. You've been more help to me than my own Dr. has been lately. Thanks again....I hope to be able to walk without pain someday.
Debbie
location unknown
Wow, that is exactly the information needed!!! thank you thank you thank you!!! I appreciate this help so very much from Marc Mitnick DPM. Excellent information and help to improve One's life.
Chrissy
location unknown
Thanks so much for this website Dr. Marc! It is so nice that you have this ask the doctor feature..I'm sure I'ts been helpful for alot of people. I will try what you suggested and see if it helps...thanks again!
Tracy
Evansville, IA
Dear Marc
I just want to say thank you for the quick response and the good info. I find it amazing and a super nice thing that you do here by answering medical questions at no charge.
Russ W.
location unknown
Your website is full of a lot of helpful information, and I am very impressed with the time in which you responded to my post. Thank you again for your time and consideration in your response.
-Sunny.
location unknown
Thank you very much for the information, I will consider it. Excellent web site.
Jackie
San Diego, CA
Dr. Mitnick, Just want to say thank you so very much for your quick response and very informative reply! After reading what you had to say, I called the doctor's office and was able to get in and see him the same day as my injury. Toe was x-rayed and luckily, it is not broken or fractured. Very badly bruised and will probably lose the toe nail. And although my toe and toe nail are still very black and blue and very sore, they ARE both starting to feel a little better. So again, thank you! I am so very happy that I came across your website. The service you provide is outstanding and immeasurable!
Rivi,
Albany, NY
Thank you so much for all of your advice. In searching the web for people dealing with this same issue i can tell you that you are a Knight In shining Armor! If I lived in Jersey I would gladly be your Spokesperson. Hopefully next time you hear from me it will be good news. God Bless,
Jill S.
location unknown
THANK YOU SO VERY MUCH FOR YOUR TIME AND EFFORTS, YOU ARE SO VERY APPRECIATED. THANK YOU FOR ALL YOU DO.
Jackie
Whichita, KS
thanks again, this site is very helpful.
mark
Boston, MA
Like others have stated...This site is amazing and I am so thankful that it was created.
....Keep up what your doing. Your a life saver.
Michelle
Colorado
Thanks again for the information provided on your site. It's easy for non-medical folk to understand your writing, and helps provide better communication between patient and doctor.
annielou
Colorado
Wonderful advice
by: Anonymous
This is the best site for foot problem info.
Thank you for this information. This description fits my pain and inflammation behind my 2nd toe perfectly.
by: Max
location unknown
Again, I really appreciate that you responded to my inquiry, and that your mention of Parkinson's helped me to find my way to a diagnosis of this difficult to diagnose disease. Most patients see on average 16 doctors before they are diagnosed. I hope that you can help other people that ask for your expertise in the future.
Barb D.
Canada
I just wanted to say that I am very greatful for this website!! I have had a fusion in my rt foot and am finally getting a little bit better......
Bonnie
location unknown
Again, Thank you from the bottom of my heart for taking the time to answer my question....your an angel!
Nancie
Wisconsin
Thank you for your response. You have provided some great insight (to my question)....
Julie
location unknown
Thank-you so very much for responding so quickly and in such detail to my question!! I will give my surgeon a call today!! This website is terrific!!!! Thank-you again!
Renae
North Carolina
Many Thanks Dr Marc!
Thank you for your response. It sounds like a good plan to me. He did not cut the wart out first ...
KG
location unknown
Thanks again doc for having this website and we STILL need qualified Podiatrists in beautiful sunny Tampa Bay (Bradenton) Florida.
Bessie Mae
Florida
Dear Dr. Mitnick, Thank you so very much for taking your time to answer my question. You have greatly relieved my anxiety related to the continual tingly I feel in my feet. I will share your response with my podiatrist next week. God bless you for having this question and answer page on your website! Most gratefully,
Lynne T.
location unknown
Your webpage is excellent, I commend you on sharing your knowledge to the public.
Robert
New Jersey
Thank you. you were more detailed than what others have told me they finally called from the last xrays and my son is now in a cast for 2 weeks he did have a fracture that was not noticeable.
a mom
location unknown
I have read your website and I have to admit that I am amazed at all the information that is on here. I have learned more than the three years I have been going to several doctors that I have seen!!
Melody
Lenoir, NC
Thank you so much Doc for a quick and thorough response!
Rustam
Bellevue, WA
I cannot thank you enough for your response, opinion, and suggestions! I want you to know how much it means to me, and I'm sure everyone else who has ever asked you a question! I feel like you're a lifesaver and have empowered me to take a stronger role and stand up for myself and my feet!
Jodi
location unknown
Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…