plantar fibromatosis
AUTHOR: Marc Mitnick DPM
REVIEWED BY: Podiatric Medical Review Board
home --> plantar fibromatosis
lump on the bottom of the foot
WHAT IS PLANTAR FIBROMATOSIS
So…. you are reading this discussion because you have this lump on the bottom of your foot and you are obviously concerned. Fact is you may have more than one lump; there may actually be a cluster of lumps.
This condition is known as plantar fibromatosis (not to be confused with plantar fasciitis) and in the vast, vast majority of cases these are benign bumps that occur on the bottom of the foot. Incidentally, a similar condition occurs on the palms of the hands known as Dupuytren’s contracture.
Plantar fibromatosis is a disorder of unknown origin. It is basically a herniation of the plantar fascia through its outer covering known as the aponeurosis. Some speculate that it is the result of tiny tears in the plantar fascia, which then undergo rapid repair, and actually over repair the area. This leads to thickened nodules ranging in size from .5cm to 3.0cm in diameter. They can then invade the dermis of the skin and sometimes the flexor tendons on the bottom of the foot making them appear even larger. These nodules may lay dormant for years only to rapidly increase in size in a very short period of time.
Note the nodular lesion in the picture below.

|
Plantar fibromatosis tend to occur more in men than women and in 25 percent of the cases are seen bilaterally.
Typically, patients will present to the office more out of concern about the lump rather than pain, but these growths can be painful. If the nodules are not painful the treatment of choice is to leave them alone.
|
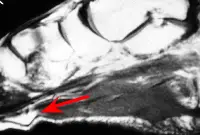
Sometimes an MRI may be helpful in an effort to show the true extent of the fibroma (red arrow) and whether or not it is pressing on adjacent tissue.
CONSERVATIVE TREATMENT OF PLANTAR FIBROMATOSIS
If, however, there is pain conservative management is indicated.
Orthopedic padding around the area in the shoe to keep pressure off the bump on the bottom of the foot. An orthotic can be very helpful in two ways. One is to keep the plantar fascial ligament from overstretching, which is considered by some to be an aggravating factor, plus the orthotic can be built in a certain manner to keep pressure off the growth. There are many soft materials which can be used as a top cover on the orthotic to protect the growth.
Night splints can be helpful in stretching the plantar fascial ligament and reducing the size of the fibroma.
Cortisone injections which in many cases shrinks them somewhat or at the very least eliminates the pain. But, I will tell you that they can be painful injections. These injections should be spaced out over a six week interval and no more than three cortisone injections should be given in a twelve month period as there are documented cases of tendon ruptures on the bottom of the foot from patients who have had more than three injections in an overall twelve month period. These injections will soften the growths which will reduce pain, but they will not make the fibroma disappear and there is a relatively high recurrence rate of painful fibromas.
Topical Verapamil- There is also available on the market a topical medication that can be applied. The histology behind plantar fibromatosis is hyper-fibroblastic activity. Fibroblasts, which are the building blocks of collagen formation, are working in overload in the case of plantar fibromatosis. It has been shown that Verapamil (a drug used in hypertension as a calcium channel blocker) can be effective when applied topically to the nodule. Since Verampamil inhibits fibroblastic activity it would make sense that the medication would work better in the early development of these lesions and would be much less effective in chronic episodes of plantar fibromatosis.
This medication is made by a group of compounding pharmacists in Texas. It has to be applied daily and over the course of six to twelve months the nodules are supposed to shrink in size. I have to say that I have not had any personal experience with the medication but I do know it is quite expensive as I inquired on behalf of a couple of patients.
Injectable Verapamil- There are some practitioners who advocate injecting 15% Verapamil directly into the lesion. Two concerns with this approach. Once again it is a painful injection directly into the lesion. (an alternate option is to do a regional anesthesia block first, then inject Verapamil directly into the lesion). The second concern is that by injecting directly into the growth the medication will not diffuse totally through the lesion which inhibits its effectiveness.
October, 2012 UPDATE Bellevue Pharmacy, a compounding pharmacy located in St. Louis, but doing business nationwide, now also offers a topical preparation for treatment of plantar fibromatosis.
I have read studies that suggest the success rate (reduction of pain and size of the growth) can be over 70 percent. It may take as long as six to twelve months of twice a day application to achieve these results, but once discontinued, the nodules may harden up once again.
If conservative measures fail and if these nodules are very painful, your only other option is surgical removal. This is not a straightforward procedure as there are many potential complications.
Experience has shown us that more than the nodule itself has to be removed. Just removing the nodule alone results in a high incidence of recurrence; I have read as high as 57%. So in order to avoid recurrence, sections of healthy plantar fascial ligament on both sides of the nodule have to also be removed. The problem here is that many times the adjacent tissue appears to be normal fascia, but histologically (at the cellular level) there is excessive fibroblastic activity which will lead to new growths. On average healthy tissue 1-2cm in length must be removed. This then creates the problem of not having use of the plantar fascial ligament whose purpose is to maintain the arch of the foot similar to the way a bowstring works on a bow and arrow. Secondly, the incision obviously has to be made on the bottom of the foot and it is generally a long curvy type incision, which opens the risk of scar formation in the incision when healed. The patient may no longer have the fibroma but they may end up with a painful scar that hurts just as much to walk.
April, 2011 UPDATE The conventional thinking has always been that these are benign lesions and can be left alone if they do not hurt. Recently I was at a lecture where the speaker mentioned that although the majority of these lesions are benign there is an incidence where lesions that appear to be fibromatosis are actually not and may have malignant tendency. That being the case, I am now going to routinely biopsy these lesions just to make sure we are only dealing with a plantar fibroma. The methods I employ are either a punch biopsy or what is known as a dry tap biopsy where a needle is inserted into the lesion and whatever aspirate comes out is sampled by the lab. Both of these methods are minimally invasive and are worth the effort.
Alternately, an MRI can be almost equally effective in ruling out malignancy of these lesions.
SURGICAL EXCISION OF PLANTAR FIBROMATOSIS
This procedure is performed using a variety of different types of incisions. Because of the potential for scarring on the bottom of the foot and because of the severe tension on the bottom of the foot when walking, a straight incision over the fibroma is usually not used.
Once the fibroma is identified it is removed along with healthy tissue on either side as to minimize recurrence. Since a large amount of plantar fascial tissue is removed, a defect is created which must be filled prior to closure.
Once closed the patient must remain non-weightbearing on the foot for around three weeks in order to allow the incision to properly heal before walking on it, in order to avoid scarring of the incision line.
The problem with this procedure is that there is a high recurrence rate and when a patient presents with multiple lumps on the bottom of the foot, surgical removal becomes more difficult.
The other issue is that the integrity of the plantar fascial ligament is weakened with this surgery and so the ligament may not function as well post-operatively. This can lead to an over-flattening of the foot.
REFERENCES

|

|

|

|

|
Want more information? CLICK HERE

Recent Articles
-
Vitamin D impact on health
Feb 06, 23 07:17 PM
Researchers are suggesting that the effectiveness of Vitamin D in fighting and preventing disease is predicated on a persons body mass index (BMI). The thinner the person the greater the positive impa… -
Foods to speed up healing
Feb 01, 23 02:41 PM
One of the best ways to help yourself heal faster after surgery is to eat well. Getting the proper nutrition will provide your body with the essentials it needs to promote healing. Here is a suggestio… -
Cancer and Type 2 Diabetes
Jan 25, 23 04:52 PM
An article revealing that older type 2 diabetics have a higher incidence of cancer then non-diabetics. It is suggested that cancer may surpass CVD as the number one cause of death in older diabetics. -
Does glucosamine or MSM reduce arthritis pain?
Jan 22, 23 01:41 PM
A good review of the possible benefits to taking glucosamine, chondroitin or MSM for arthritis. Always beware of the possible side effects of over the counter supplements. -
shin splints
Jan 18, 23 05:12 PM
A great review on the various causes of shin splints, along with treatment options. -
Whats new in skin cancer?
Jan 15, 23 08:32 PM
A presentation of newer skin protection combinations in an effort to better protect the skin from the hazards of sun exposure. -
Causes and risk factors of warts
Jan 14, 23 05:02 PM
A good review of the causes of warts and protective measures you can take to prevent developing them. -
Do chronic wounds need to be dressed daily?
Jan 11, 23 02:18 PM
Because of supply chain shortages as well as staffing shortages particularly during the pandemic, many institutions extended the time between dressing changes for chronic wounds. Is this really the be… -
Food choices that raise your risk of type 2 diabetes
Jan 08, 23 10:07 AM
A good review of how blood sugars can become elevated and the harm that can do. Certain food groups have a tendency to raise your blood sugars and should be avoided. -
Outcome stats from Scarf bunionectomy
Jan 03, 23 03:04 PM
The Journal of Foot and Ankle Surgery recently reported a meta analysis of outcomes in 1583 Scarf bunionectomies that met their inclusion criteria. Adverse events did not seem to be any better or wors…